-
PhoneOximeter
Pulse oximetery on a cell phone
Contact Person In poorer parts of the world, most preventable anesthesia morbidity and mortality is related to airway and respiratory problems leading to lack of oxygen (hypoxia). A pulse oximeter gives an early warning of hypoxia by monitoring the percentage of hemoglobin in the blood that is oxygenated. An early, rapid and effective response to early signs of hypoxia, detected and displayed by a pulse oximeter, can rescue the patient from the permanent effects of lack of oxygen, such as brain damage or death.
In poorer parts of the world, most preventable anesthesia morbidity and mortality is related to airway and respiratory problems leading to lack of oxygen (hypoxia). A pulse oximeter gives an early warning of hypoxia by monitoring the percentage of hemoglobin in the blood that is oxygenated. An early, rapid and effective response to early signs of hypoxia, detected and displayed by a pulse oximeter, can rescue the patient from the permanent effects of lack of oxygen, such as brain damage or death.
In this project, we propose to develop and evaluate a wireless pulse oximeter that uses a cell phone to analyze the information received from a sensor placed on the finger. The inherent capabilities of a standard cell phone (which are widely available in underdeveloped areas) will be used to intelligently analyze and creatively communicate information from the sensor. The primary goal of this project is to demonstrate the potential for enhanced delivery of information from a pulse oximeter to enhance the safety of anesthesia care throughout the world.
See: World Health Organization Global Pulse Oximetry Project -
Post-Discharge Survival
Reducing mortality and morbidity of under 5 year olds discharged from hospital in Uganda
Contact Person In Sub-Saharan Africa, infectious disease accounts for 6.3 million deaths among children under 5 years old. Postdischarge death is recognized as a major contributor to overall child mortality. These deaths occur within several weeks of hospital discharge, and this research aims to reduce the rates of mortality using a discharge bundle consisting of 3 components. Firstly, the PAediatric Risk Assessment mobile application is used along with a pulse oximeter to identify pediatric patients at high risk of both in-hospital and postdischarge mortality. Secondly, a discharge kit provides education on post-discharge risk periods and recognizable early warning signs of recurrent illness. The kit also includes health incentives such as a bed net, soap and oral rehydration salts. Lastly, a back-referral to a village health center ensures that high risk children are seen by a health provider in the critical days and weeks following discharge. Recurrent illness is more easily recognized and critical cases can be referred back to hospitals.
In Sub-Saharan Africa, infectious disease accounts for 6.3 million deaths among children under 5 years old. Postdischarge death is recognized as a major contributor to overall child mortality. These deaths occur within several weeks of hospital discharge, and this research aims to reduce the rates of mortality using a discharge bundle consisting of 3 components. Firstly, the PAediatric Risk Assessment mobile application is used along with a pulse oximeter to identify pediatric patients at high risk of both in-hospital and postdischarge mortality. Secondly, a discharge kit provides education on post-discharge risk periods and recognizable early warning signs of recurrent illness. The kit also includes health incentives such as a bed net, soap and oral rehydration salts. Lastly, a back-referral to a village health center ensures that high risk children are seen by a health provider in the critical days and weeks following discharge. Recurrent illness is more easily recognized and critical cases can be referred back to hospitals. -
Interrupting Pathways to Sepsis
mHealth tools for identifcation of children needing hospitalization
Contact Person
Funded by the Canadian Government's Muskoka Initiative, Interrupting Pathways to Maternal, Newborn and Early Childhood Sepsis Initiative (IPSI) was designed with the objective of improving maternal and child survival by interrupting pathways to sepsis. The ECEM team's role within this project is to produce mHealth tools that identify sepsis and provide decision support for community healthcare workers. Data were collected from 3374 children under the age of 5 presenting at a tertiary care hospital in Bangladesh. With this data, predictive models were created to predict the need for hospitalization. These models must now be externally validated in a community setting. -
Community Level Interventions for Pre-eclampsia
Predicting adverse outcomes in pregnancy
Contact Person The hypertensive disorders of pregnancy (HDP), including pre-eclampsia, remain one of the top three categories of maternal mortality and morbidity, globally. The majority of deaths due to HDP occur in low and middle income countries. The Community Level Interventions for Pre-eclampsia (CLIP) trial is a large cluster randomised controlled trial happening in Mozambique, Pakistan and India using mobile applications developed by the ECEM group. Community healthcare workers use the CLIP PIERS on the Move mobile application to regularly assess pregnant women in their homes. The app uses the mini-PIERS (Pre-eclampsia Integrated Estimate of RiSk) predictive model to determine the probability of an adverse event in the next 48 hours and then provide a recommendation of regular care or antihypertensives and transport to a hospital.
The hypertensive disorders of pregnancy (HDP), including pre-eclampsia, remain one of the top three categories of maternal mortality and morbidity, globally. The majority of deaths due to HDP occur in low and middle income countries. The Community Level Interventions for Pre-eclampsia (CLIP) trial is a large cluster randomised controlled trial happening in Mozambique, Pakistan and India using mobile applications developed by the ECEM group. Community healthcare workers use the CLIP PIERS on the Move mobile application to regularly assess pregnant women in their homes. The app uses the mini-PIERS (Pre-eclampsia Integrated Estimate of RiSk) predictive model to determine the probability of an adverse event in the next 48 hours and then provide a recommendation of regular care or antihypertensives and transport to a hospital. -
Closed Loop Control in Anesthesia
Contact Person Computer controlled, or automatic, drug delivery is the process of administering a therapeutic regime to a patient with computer assistance for calculation of optimal dose and delivery schedules. Computer control can improve drug therapy by reducing drug usage and costs, by permitting health care staff to work more efficiently and to provide better standard of care, by allowing the safe use of drugs that are difficult to administer, and by compensation for human failings with computer strengths, such as unlimited attention span and patience, and capacity for quick, accurate and redundant calculation. Our goal is to develop an automatic control system for anesthesia and to demonstrate its efficacy, safety and benefits in an operating room. Although closed-loop anesthesia has previously been proposed and tested, it has yet to have a significant impact on clinical practice. Recent developments in sensing for anesthesia have opened new possibilities for ‘closing the loop’. Our research will focus on the deployment of new sensors optimized for controlled drug delivery, robust control methodology and extensive clinical validation. In addition, through advanced control techniques, we aim to provide a mathematical guarantee of the safety of patients under anesthesia.
Computer controlled, or automatic, drug delivery is the process of administering a therapeutic regime to a patient with computer assistance for calculation of optimal dose and delivery schedules. Computer control can improve drug therapy by reducing drug usage and costs, by permitting health care staff to work more efficiently and to provide better standard of care, by allowing the safe use of drugs that are difficult to administer, and by compensation for human failings with computer strengths, such as unlimited attention span and patience, and capacity for quick, accurate and redundant calculation. Our goal is to develop an automatic control system for anesthesia and to demonstrate its efficacy, safety and benefits in an operating room. Although closed-loop anesthesia has previously been proposed and tested, it has yet to have a significant impact on clinical practice. Recent developments in sensing for anesthesia have opened new possibilities for ‘closing the loop’. Our research will focus on the deployment of new sensors optimized for controlled drug delivery, robust control methodology and extensive clinical validation. In addition, through advanced control techniques, we aim to provide a mathematical guarantee of the safety of patients under anesthesia. -
VitalPAD
An intelligent monitoring and communication device to optimize safety in the Pediatric Intensive Care Unit
Contact Person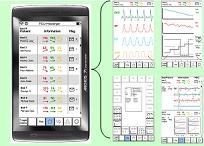 The goal is to develop a unified, portable and intelligent device that integrates information from multiple patient monitors, mechanical ventilators, infusion pumps and clinical information systems. It will allow PICU healthcare team members, on or off-site, to monitor critically ill patients continuously. The project involves two components: a) We will use feedback obtained in a participatory design process to guide the development of the VitalPAD, and b) We will use simulated ICU scenarios, to evaluate whether clinicians will prioritize the care of critically ill patients more rapidly and more accurately with the use of VitalPAD than without it.
The goal is to develop a unified, portable and intelligent device that integrates information from multiple patient monitors, mechanical ventilators, infusion pumps and clinical information systems. It will allow PICU healthcare team members, on or off-site, to monitor critically ill patients continuously. The project involves two components: a) We will use feedback obtained in a participatory design process to guide the development of the VitalPAD, and b) We will use simulated ICU scenarios, to evaluate whether clinicians will prioritize the care of critically ill patients more rapidly and more accurately with the use of VitalPAD than without it. -
Anesthesia in Neonates
Vital signs changes in neonates during general anesthesia: an objective method to compare cases
Contact Person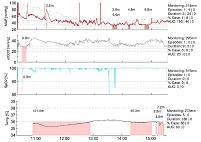 General anesthesia in neonates has the potential to impair long term cognitive outcomes. However, given that anesthesia for urgent neonatal surgery cannot be avoided regardless of age, it is vitally important to understand the other factors that may contribute to poor long term outcomes. Attention is now directed to preventable factors such as changes in vital signs, which may have deleterious effects on cerebral perfusion in the neonatal brain. The goal of this research is to identify and prioritize rules for detecting vital sign deviations, and to develop a case severity score allowing comparison of cases with respect to the conduct of anesthesia. This tool will then be used to support future quality improvement projects and to facilitate future investigations into the conduct of neonatal anesthesia applied in multi-centre prospective studies.
General anesthesia in neonates has the potential to impair long term cognitive outcomes. However, given that anesthesia for urgent neonatal surgery cannot be avoided regardless of age, it is vitally important to understand the other factors that may contribute to poor long term outcomes. Attention is now directed to preventable factors such as changes in vital signs, which may have deleterious effects on cerebral perfusion in the neonatal brain. The goal of this research is to identify and prioritize rules for detecting vital sign deviations, and to develop a case severity score allowing comparison of cases with respect to the conduct of anesthesia. This tool will then be used to support future quality improvement projects and to facilitate future investigations into the conduct of neonatal anesthesia applied in multi-centre prospective studies. -
Temperature feedback
Using thermoregulation metrics during scoliosis correction surgery as an example for team and individualized feedback mechanisms
Contact Person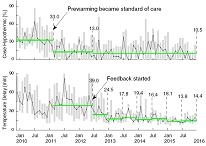 Unless something is measured, practitioners don’t know how they are doing and where improvements are needed. Engaging high-performing individuals’ desire to do better is not always readily achieved by checklists, policies or guidelines. Continuous feedback of performance data can improve professional practice and outcomes. In this study, feedback of thermoregulation metrics is used as one strategy to continuously improve perioperative temperature management in our scoliosis patients. Individualized feedback, without changes in policy, is able to reduce monitoring delays significantly, and sustainably.
Unless something is measured, practitioners don’t know how they are doing and where improvements are needed. Engaging high-performing individuals’ desire to do better is not always readily achieved by checklists, policies or guidelines. Continuous feedback of performance data can improve professional practice and outcomes. In this study, feedback of thermoregulation metrics is used as one strategy to continuously improve perioperative temperature management in our scoliosis patients. Individualized feedback, without changes in policy, is able to reduce monitoring delays significantly, and sustainably. -
Tissue oxygen saturation in malnutrition and pnemonia
Using NIRS technology to measure tissue oxygen saturation
Contact Person
Founded by Grand Challenges Exploration, this study is one of our ongoing global health projects in Uganda, Africa. Children with moderate to severe malnutrition are more susceptible to get infections creating a vicious cycle of “infection-malnutrition”. Near Infrared Spectroscopy (NIRS) is a non-invasive technology which could be used in clinical settings to measure changes in tissue oxygenation and hemodynamics. The purpose of this study is to evaluate and develop a non-invasive diagnostic and treatment-progress monitoring tool to assess peripheral muscle oxygen saturation levels using NIRS. The absorption of very specific wavelengths of light in a child will provide an objective measure of a child’s metabolic status and allow identification of those who are at increased risk of dying from pneumonia. This method will assess disease severity and monitor treatment progress.
Project Websites
News
-
2017-12-11
New Digital Health Innovation Lab websiteThe Digital Health Innovation Lab now has a new website: https://bcchr.ca/dhil/
-
2017-02-24
Guy Dumont wins NSERC Synergy Award for InnovationGuy Dumont has received an NSERC Synergy Award for Innovation in the category of small- and medium-sized companies. Valued at $200,000, the award recognizes superior university-industry...
-
2017-01-17
Personalized feedback research featured at BC Children's HospitalBC Children's Hospital Research Institute shared a story of How...
-
2016-09-01
Research featured in the mediaWork from Zoya Bastany's MASc thesis reported in local media. Link...